Immotile Cilia Syndrome (Kartagener's Trial)



posted by tvnkamal @ 11:18 AM
0 Comments
![]()



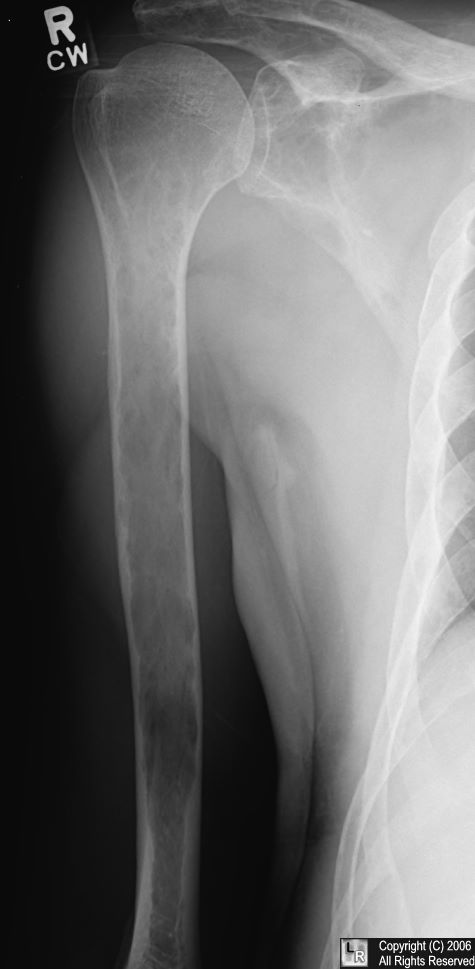
Multiple myeloma . The pelvis contains numerous lytic lesions without reactive sclerosis which
have an almost "soap-bubbly" appearance in the ischia. There are also lytic lesions in
both proximal femora.
Other examples of Multiple Myeloma (Click on each to enlarge)



posted by tvnkamal @ 11:17 AM
0 Comments
![]()
 | What is Galactography?Galactography, or ductography, is a mammographic technique that involves injection of a contrast agent (dye) into a milk duct. This study may be useful in the evaluation of unilateral spontaneous nipple discharge that is bloody. (Nipple discharge that is milky, yellow, or green is rarely associated with breast cancers.)
What can I expect from the examination?The initial radiologic evaluation of nipple discharge includes a mammogram. If no abnormality is visible, a galactogram may be indicated. The duct must be discharging on the day of the study in order to identify the correct orifice to be cannulated. A tiny blunt-tipped catheter (called a cannula) is inserted into the discharging duct and a small (approximately 1 ml) amount of contrast agent is injected. Additional mammographic images are obtained. Some patients report a sensation of "fullness" during the examination, but no sharp pain or burning should be experienced. If an abnormality is detected on the galactogram, surgical excision is recommended.The most common cause of abnormal nipple discharge is a papilloma (a benign tumor that grows from the wall of a duct). Fewer than 10% of patients with abnormal duct discharge have a related breast malignancy. |
The figure to the left is a galactogram. Note that the contrast material dramatically increases the visibility of the ducts. |
posted by tvnkamal @ 11:15 AM
0 Comments
![]()
| Medical Centers near The Belamar. |  | |||||||||
|
posted by tvnkamal @ 8:13 AM
0 Comments
![]()

 The College of Medicine’s goal is the broad preparation of students to practice medicine. Regardless of eventual specialty selection, students must demonstrate competence in those intellectual, physical, and social tasks that together represent the fundamentals of medical practice. Applicants and students will be judged not only on their scholastic achievement and ability,but also on their intellectual, physical, and emotional capacities to meet the full requirements of the school’s curriculum. As an advisory committee to the Dean, the Admissions Committee is instructed to exercise judgment on behalf of the faculty members to recommend the entering class, and to consider character, extracurricular achievement, and overall suitability for the medical profession on the basis of information in the application, letters of recommendation, and personal interviews.
The College of Medicine’s goal is the broad preparation of students to practice medicine. Regardless of eventual specialty selection, students must demonstrate competence in those intellectual, physical, and social tasks that together represent the fundamentals of medical practice. Applicants and students will be judged not only on their scholastic achievement and ability,but also on their intellectual, physical, and emotional capacities to meet the full requirements of the school’s curriculum. As an advisory committee to the Dean, the Admissions Committee is instructed to exercise judgment on behalf of the faculty members to recommend the entering class, and to consider character, extracurricular achievement, and overall suitability for the medical profession on the basis of information in the application, letters of recommendation, and personal interviews.

Students must be able to observe demonstrations and to conduct experiments in the basic sciences, including but not limited to physiologic and pharmacologic demonstrations in animals, microbiologic cultures, and microscopic studies of microorganisms and tissues in normal and pathologic states. A student must be able to observe a patient accurately at a distance and close at hand, noting nonverbal and verbal signals.  Specific vision-related requirements include but are not limited to the
Specific vision-related requirements include but are not limited to the
following abilities: skin, culture media, and dipstick tests; visualizing and discriminating findings on x-rays and other imaging tests; reading written and illustrated material; observing demonstrations in the classroom, including projected slides and overheads; observing and differentiating changes in body movement; observing anatomic structures; discriminating numbers and patterns associated with diagnostic instruments and tests, such as sphygmomanometers and electrocardiograms; and using instruments competently, such as stethoscope, otoscope, ophthalmoscope, and microscope.
posted by tvnkamal @ 8:10 AM
0 Comments
![]()

The Medical Physics Group is primarily based at the Radiation Oncology Department, Newcastle Mater Hospital (NMH) and have conjoint appointments with the University of Newcastle. The group is concerned with the physics that underlies the practice of radiation therapy for the treatment of cancer and have a strong track record in dosimetry research. Our research interests fall into the following broad topic ranges (see individual pages for more details):
We also have active clinical treatment and development programs including IMRT, HDR brachytherapy, MRI and PET in treatment planning, and fiducial marker guided prostate treatment.
Enquiries from prospective students are welcome. Please contact Peter Greer or Martin Ebert
posted by tvnkamal @ 8:09 AM
0 Comments
![]()

Subscribe to
Comments [Atom]